Myopia (nearsightedness) has reached epidemic proportions in the 21st century, driven by lifestyle shifts towards prolonged near-work and digital screen exposure. This article explores the personal and public health implications of myopia, debunking common myths surrounding refractive surgery (LASIK) and highlighting the critical role of nutrition and behavioral habits in disease progression. By synthesizing personal narrative with medical research, we argue for a preventative approach centered on the "20-20-20" rule and dietary awareness.
My experience with myopia has been defined by the constant, subtle pressure of frames against my temples—a perpetual reminder of a barrier between myself and the world. Many describe corrective lenses as a simple tool, but for those of us who rely on them daily, they can feel like a foreign object. Contact lenses, often touted as the invisible alternative, present their own challenges, directly pressing onto the eye and requiring a level of desensitization that not everyone can master.
The rapid deterioration of eyesight, particularly myopia (nearsightedness), often occurs during the critical developmental windows of childhood and adolescence. My own journey mirrors a common narrative in the digital age: a childhood prioritized around screens—gaming, binge-watching television—at the expense of ocular health.
1. The Anatomy of Vision: How We See
To understand how digital strain affects our eyes and causes conditions like myopia, it is crucial to first understand the complex mechanics of normal human vision. Our eyes are intricate optical instruments that rely on a precise coordination of anatomical structures to capture light and convert it into the images we perceive.
1.1 The Pathway of Light
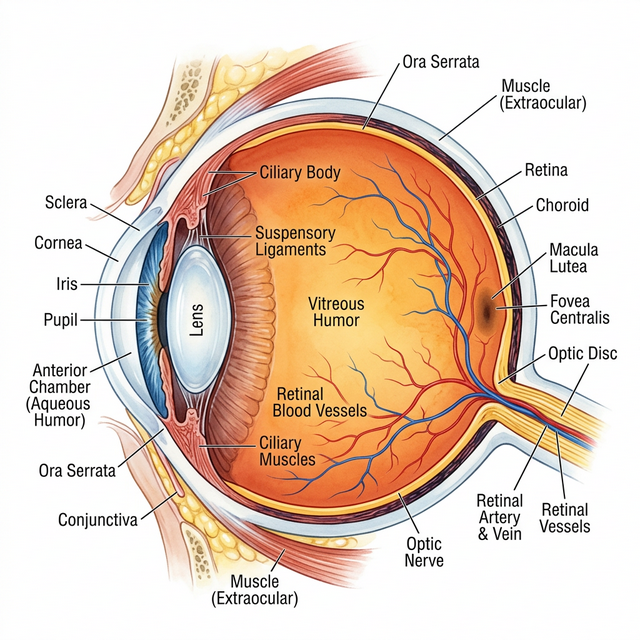
The process of vision begins when light bounces off an object and enters the eye. The journey of that light passes through several key structures:
- Tear Duct (Lacrimal Apparatus): While not directly involved in focusing light, the tear system maintains the optical clarity of the cornea by keeping it lubricated, smooth, and free of debris.
- Cornea: This clear, dome-shaped front surface of the eye acts as the primary lens. It provides about 65-75% of the eye's focusing power, bending (refracting) the incoming light rays through the pupil.
- Lens: Sitting just behind the pupil, the crystalline lens provides the fine-tuning focusing power. It changes shape to help focus light precisely onto the back of the eye, a process known as accommodation.
- Ciliary Muscles: These tiny muscles control the shape of the lens. When we look at something close (like a phone screen), the ciliary muscles contract to make the lens thicker, increasing its focusing power. Prolonged contraction of these muscles is a primary cause of digital eye strain.
1.2 Photoreception and Neural Conversion
Once light has been focused by the cornea and lens, it hits the Retina, the light-sensitive tissue lining the inner surface of the back of the eye. The center of the retina, known as the Macula, is responsible for our sharpest, most detailed central vision.
The retina contains millions of specialized sensory cells called photoreceptors, which come in two main types:
- Rods: Highly sensitive to light and motion, rods allow us to see in low-light conditions (scotopic vision) but do not process color or fine detail.
- Cones: Concentrated heavily in the macula, cones require brighter light to function and are responsible for our color vision and high visual acuity (ability to see fine detail).
When light hits these photoreceptors, it triggers a chemical reaction that converts the light energy into electrical signals. This is where the complex neural network of the eye takes over:
- Bipolar Cells: These intermediate neurons act as a bridge. They gather the electrical signals generated by the rods and cones and pass them forward.
- Ganglion Cells: The bipolar cells transmit the signals to the retinal ganglion cells. These cells serve as the final output neurons of the retina.
- The Optic Nerve: The long, cable-like extensions (axons) of all the ganglion cells bundle together to form the optic nerve. This nerve acts as the high-speed data cable transmitting the visual information from the eye directly to the brain's visual cortex for processing.
1.3 The Mechanics of Refractive Error
Perfect vision (emmetropia) occurs when the cornea and lens focus light rays precisely on the surface of the retina. However, when the physical shape of the eye deviates from the norm, it results in a refractive error.
Light focuses precisely on the retina.
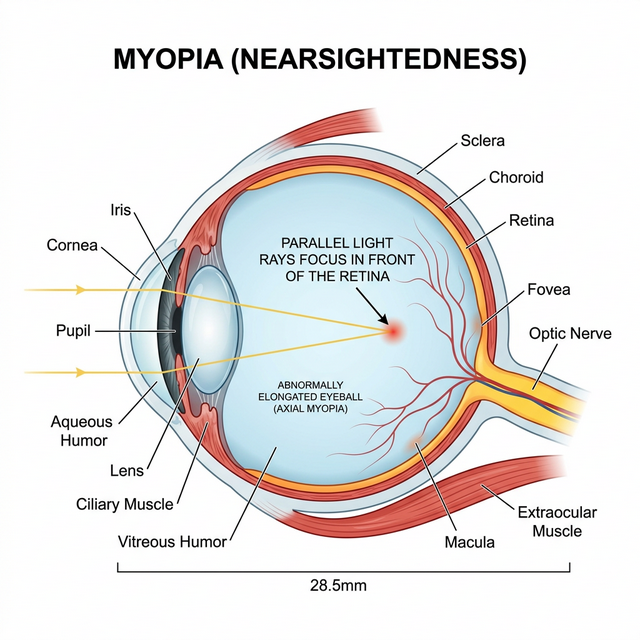
An elongated eyeball causes light to focus in front of the retina, blurring distant objects.
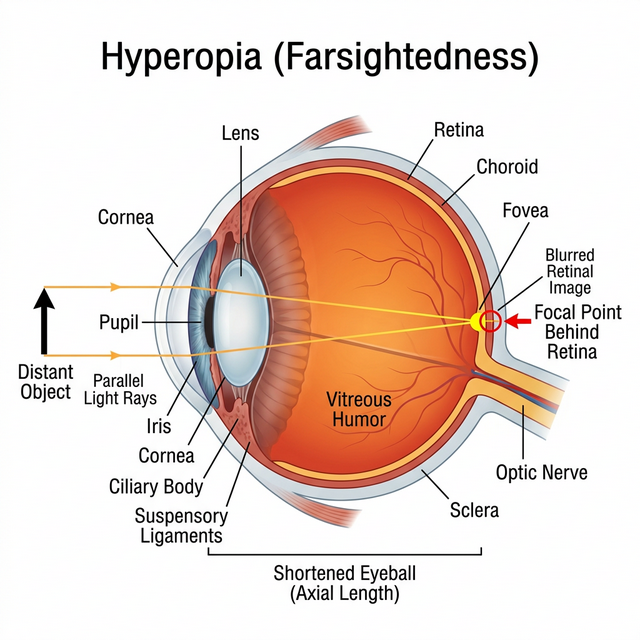
A shortened eyeball causes light to focus behind the retina, straining near vision.
2. The "Normalized" Strain
We live in an era where digital dependency is not just common; it is required. From educational tools to social connection, removing screens entirely is not a pragmatic solution. However, the abuse of screens—using them for elongated periods without breaks—is the catalyst for damage.
As a child, I dismissed the warnings of my parents. I ignored the 20-20-20 rule (look at something 20 feet away for 20 seconds every 20 minutes) and the deterioration was swift. It is a misconception that eye strain alone causes myopia; rather, it is the habitual signaling to the life, the damage done during developmental years is often exponential and irreversible.
2.1 The Dose-Response Reality
A recent systematic review and meta-analysis of 45 studies involving over 335,000 participants has quantified the risk of digital exposure [5]. The findings reveal a "sigmoidal" (S-shaped) relationship between screen time and myopia progression:
- 0 to 1 Hour (Safety Threshold): The risk remains statistically insignificant.
- 1 to 4 Hours (The Spike): The probability of developing myopia rises dramatically.
- Over 4 Hours (Saturation): The risk continues to increase, though the rate of acceleration slows.
Crucially, the study identified a 21% increase in myopia odds for every additional hour of daily screen time. This is particularly concerning given the explosion in global smartphone usage, which jumped from 21.6% in 2014 to 69.0% in 2023, with children as young as two years old now regularly engaging with devices.
2.2 Global Trajectory & Pathologic Risks
The prevalence of myopia currently exceeds 28.3% globally and is projected to affect 50% of the world's population by 2050 [6]. More alarming is the rise of "High Myopia," expected to impact 10% of the global demographic. Beyond simple blurriness, high myopia is linked to irreversible pathologic conditions:
- Retinal Detachment: Increased axial length stretches the retina, thinning it to the point of tearing.
- Glaucoma & Cataracts: significantly higher incidence rates in myopic eyes.
- Myopic Macular Degeneration (MMD): A leading cause of untreatable blindness.
3. The Surgical Myth: LASIK is Not a "Reset"
Many adolescents view refractive surgery, such as LASIK, as a guaranteed "cure-all" waiting for them in adulthood. This is a dangerous fallacy. Refractive surgery is not a simple reset button; it is a complex medical procedure with strict biological limitations.
3.1 The Age Factor. While technically approved for adults over 18, most ethical surgeons heavily recommend waiting until the mid-twenties (ages 23–25). Why? The eye must be refractively stable. Operating on an eye that is still changing is futile, as the myopia can progress post-surgery.
3.2 The "One-Shot" Reality. There is a common belief that one can simply get LASIK "touched up" repeatedly. In reality, LASIK involves slicing a thin flap of the cornea and ablating the tissue underneath. Corneal thickness is a finite resource. Once that tissue is removed, it does not grow back. While enhancements are possible in some cases, the eye cannot be structurally comprised indefinitely. For many, LASIK is a one-time opportunity, and managing your eye health before surgery is crucial to being a candidate at all.
4. Lifestyle & Nutrition: The Hidden Link
Beyond screens, our physiological choices play a pivotal role. The "Western Diet"—high in processed foods, refined carbohydrates, and sugars—has been linked to the acceleration of myopia.
High-glycemic diets can spike insulin levels, which may lead to an increase in insulin-like growth factor-1 (IGF-1). This hormone can signal the eye to grow axially (elongate), worsening nearsightedness. If you believe your vision is stable at -2.00 diopters, consider the functional difference of -4.00 or -6.00. At higher prescriptions, the world without glasses is not just blurry; it is unrecognizable. Faces fade, items blend into surroundings, and functional independence is lost. Preserving your vision at its current stage is not just about avoiding thicker glasses—it is about maintaining quality of life.
5. Strategic Interventions: Clinical vs. Behavioral
As the crisis deepens, the debate between clinical pharmaceutical intervention and behavioral modification intensifies.
5.1 Clinical Interventions
As the myopia epidemic intensifies, the reliance on traditional glasses and daytime contact lenses is shifting. Standard corrective lenses merely compensate for the refractive error (blurriness) without addressing the underlying structural elongation of the eye. Modern clinical interventions distinguish themselves by actively aiming to slow physical eye growth (Axial Length).
Orthokeratology (Ortho-K)
Orthokeratology involves wearing specially designed, rigid gas-permeable contact lenses overnight. These lenses gently reshape the cornea while the patient sleeps, temporarily flattening the center.
- Pros: The primary benefit is highly effective myopia control—studies show Ortho-K significantly reduces the rate of axial elongation [1]. Furthermore, it grants patients clear, unassisted vision throughout the day, which is invaluable for active adolescents and athletes. It is also non-surgical and entirely reversible.
- Cons: The treatment demands strict compliance with overnight wear and diligent lens hygiene. Because the lens is worn during sleep, there is a slightly elevated risk of adverse events, primarily microbial keratitis (corneal infection), compared to daily disposable lenses [5]. Additionally, if treatment is abruptly stopped, the eye's growth rate can rebound.
Atropine Therapy
Atropine eye drops, used in very low concentrations (e.g., 0.01% to 0.05%), have become a frontline pharmaceutical defense against progressive myopia. Unlike Ortho-K, they do not correct daytime vision, so the patient must still wear glasses or contacts.
- Pros: Low-dose Atropine is widely considered one of the most effective and easily administered methods for slowing axial length growth in children, demonstrating a strong safety profile in long-term studies.
- Cons: Side effects can include mild photophobia (light sensitivity) due to slight pupil dilation and reduced accommodative ability (blurriness when reading up close). Like Ortho-K, a rebound effect is possible upon discontinuation, necessitating a gradual tapering process.
5.2 Behavioral Interventions (Outdoor Time)
Myopia is a complex condition caused by a mix of our genetics and our environment. Over the last 30 years, the number of adolescents needing glasses has skyrocketed globally. This suggests that the way we live today—spending more time on screens and less time outside—is directly harming our vision.
Why the Sun Matters
Scientific studies on both humans and animals have shown a clear pattern: being outside in natural light helps protect a child's eyes. While we know that being outdoors helps prevent myopia from starting, researchers are still studying exactly how much it helps stop myopia from getting worse once it has already developed.
How Does It Work?
Scientists have a few theories on why natural light is the "secret weapon" for eye health:
- Dopamine Boost: Bright light might trigger the release of dopamine in the eye, which acts like a signal to stop the eye from growing too long (the primary cause of blurry distance vision).
- The "Focus" Effect: High levels of ambient light make our pupils smaller, creating a sharper image on the retina and reducing "visual blur."
- Light Quality: Exposure to specific types of light (such as shorter wavelengths) found outdoors may play a crucial role in healthy eye development.
• Reduced Blink Rate
• Blue Light Exposure
• Look 20 Feet Away
• For 20 Seconds
Note: This mechanism relaxes the ciliary muscle inside the eye, reducing accommodative fatigue.
6. Glossary of Terms
- Cornea
- The clear, dome-shaped front surface of the eye that provides most of the eye's focusing power.
- Lens
- The transparent structure behind the pupil that changes shape to fine-tune focus on objects at various distances.
- Ciliary Muscles
- Tiny muscles that control the shape of the lens for focusing. Prolonged contraction causes digital eye strain.
- Retina
- The light-sensitive tissue lining the back of the eye that converts light into electrical signals.
- Macula
- The small central area of the retina responsible for sharp, detailed, and central vision.
- Rods and Cones
- Photoreceptor cells in the retina. Rods handle low-light and motion vision. Cones handle color and fine detail.
- Bipolar and Ganglion Cells
- Neural cells in the retina that process signals from photoreceptors and pass them to the optic nerve.
- Tear Duct
- Part of the lacrimal system that produces tears to keep the cornea lubricated and clear.
- Axial Length (AL)
- The physical length of the eye from front to back. A longer AL is the primary indicator of more severe myopia.
- Spherical Equivalent Refraction (SER)
- The standard measurement for prescription strength. Myopia is generally defined as an SER of ≤ -0.50 diopters (D).
- Atropine
- A pharmaceutical eye drop used to dilate the pupil and paralyze the accommodation mechanism, often used off-label to slow myopia progression.
- Orthokeratology (Ortho-K)
- Rigid gas-permeable contact lenses worn overnight to reshape the cornea temporarily.
- High Myopia
- Severe nearsightedness (usually > -6.00 D) associated with pathologic risks like retinal detachment.
7. Conclusion
Myopia is not merely a functional inconvenience fixed by a stronger prescription; it is a structural deformation of the eye. The elongation of the axial length is irreversible, making prevention from the onset the most critical strategy we have.
Failing to arrest this progression in childhood and adolescence directly paves the way for High Myopia in adulthood. The consequences of high myopia are severe and sight-threatening. A stretched, thinned retina is highly susceptible to tearing and Retinal Detachment. The altered ocular biomechanics drastically elevate the lifetime risk of developing Glaucoma, and the sheer tension at the back of the eye can trigger Myopic Macular Degeneration (MMD)—conditions that lead to permanent, untreatable vision loss.
Whether the intervention relies on clinical therapies like Ortho-K and Atropine, or behavioral modifications like the 20-20-20 rule and increased outdoor time, the goal remains the same: stop the elongation before it reaches a critical threshold. A proactive, preventative approach today is the only definitive way to preserve quality of life and ocular integrity for tomorrow.
References
- Holden, B. A., et al. (2016). Global Prevalence of Myopia and High Myopia and Time Trends from 2000 through 2050. Ophthalmology.
- Cordain, L., et al. (2002). An evolutionary analysis of the aetiology and pathogenesis of juvenile-onset myopia. Acta Ophthalmologica Scandinavica.
- American Optometric Association. (n.d.). Computer Vision Syndrome.
- FDA. (2023). LASIK Quality of Life Collaboration Project.
- Tang, S. M., et al. (2024). Digital Screen Time and Myopia Among Children and Adolescents. JAMA Network Open.
- Li, M., et al. (2024). Outdoor Interventions for Myopia Control: A Systematic Review. Frontiers in Public Health.
- Baird, P. N., et al. (2020). Myopia. Nature Reviews Disease Primers (PMC9305934). Available here.